

What is glutaryl-CoA dehydrogenase deficiency glutaric acidemia type 1?
Glutaric acidemia type 1 (GA1) is an inherited metabolic disorder. It arises when the body cannot effectively break down certain amino acids—the building blocks of protein—due to a deficient enzyme. This leads to an accumulation of specific harmful acidic substances in the body, particularly affecting the brain and potentially causing significant health issues. The severity and presentation of GA1 can differ widely among individuals.
Key aspects of this condition include:
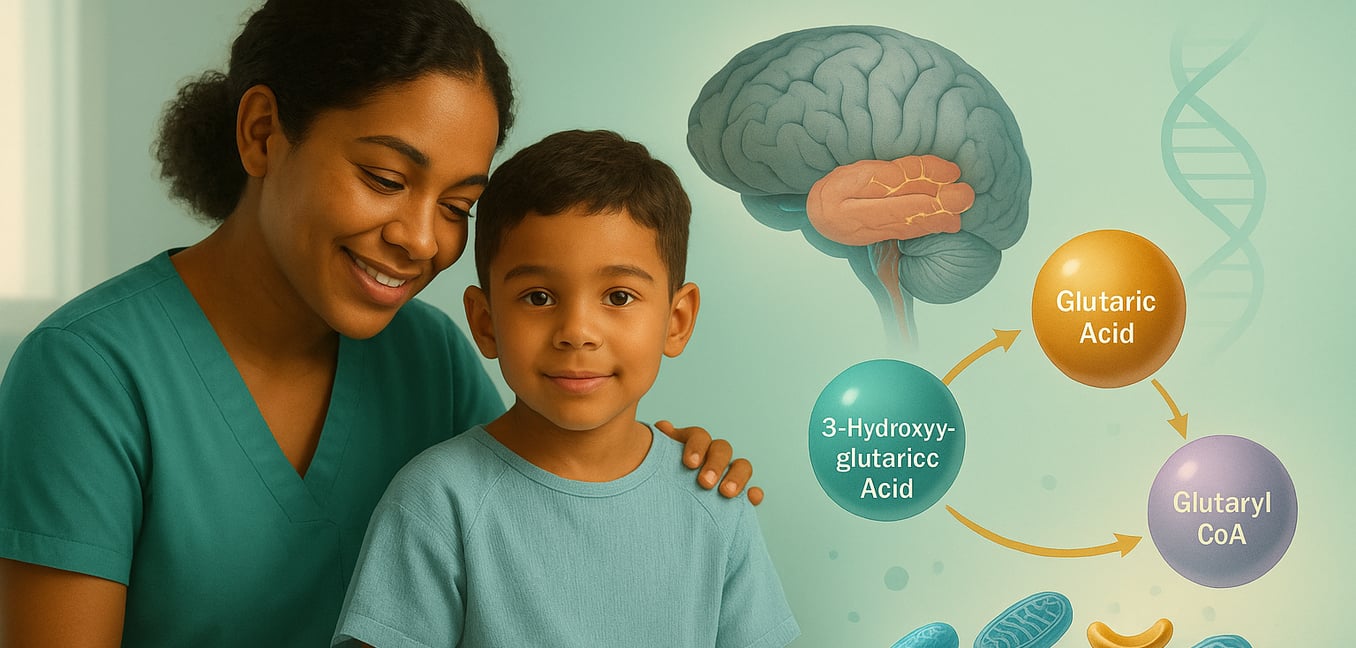
- Core Cause : GA1 is caused by a deficiency of the enzyme glutaryl-CoA dehydrogenase (GCDH). This enzyme is essential for processing three amino acids: lysine, hydroxylysine, and tryptophan. Mutations in the GCDH gene disrupt this process, leading to a harmful buildup of intermediate compounds.
- Neurological Impact : The accumulation of these unprocessed substances is toxic, especially to a brain region called the basal ganglia, which is crucial for movement control. This can result in neurological problems such as involuntary movements, muscle stiffness, or reduced muscle tone. However, with early diagnosis and consistent treatment, many individuals can maintain normal intellectual development.
- Early Indicators and Crises : Some infants with GA1 may present with an unusually large head (macrocephaly). Often, more distinct symptoms emerge during infancy or early childhood, frequently triggered by bodily stress like illness or fever. These events can precipitate "encephalopathic crises"—sudden episodes of neurological decline—which can lead to lasting brain injury if not managed promptly.
The Genetic and Enzymatic Basis of GA1
Glutaric Acidemia Type 1 is fundamentally a genetic disorder that impairs a crucial metabolic pathway due to a specific enzyme deficiency. Understanding its genetic and enzymatic roots is key to comprehending the condition.
- The GCDH Gene and Enzyme : GA1 results from mutations in the GCDH gene. This gene holds the instructions for producing the enzyme glutaryl-CoA dehydrogenase. This enzyme plays a vital role in the breakdown pathway of the amino acids lysine, hydroxylysine, and tryptophan. When the GCDH gene is mutated, the body either produces an insufficient amount of the enzyme, or the enzyme produced is defective and cannot function correctly.
- Inheritance Pattern : GA1 is inherited in an autosomal recessive manner. This means that an affected child must inherit two copies of the mutated GCDH gene, one from each parent. Parents who carry one mutated copy are known as carriers; they typically do not exhibit symptoms of GA1 but have a 25% chance with each pregnancy of having a child with the condition.
- Consequences of Enzyme Deficiency : The deficiency of glutaryl-CoA dehydrogenase blocks the metabolic processing of glutaryl-CoA, an intermediate product in the breakdown of the aforementioned amino acids. Consequently, glutaryl-CoA and related compounds, such as glutaric acid and 3-hydroxyglutaric acid, accumulate to toxic levels. This buildup is particularly damaging to the brain's basal ganglia, leading to the neurological symptoms characteristic of GA1.
- Enzyme Activity Variation : Individuals with GA1 can have varying levels of residual enzyme activity. Some, termed "low excretors," might retain up to 30% of normal glutaryl-CoA dehydrogenase activity, resulting in lower urinary excretion of glutaric acid. Others, "high excretors," have minimal to no enzyme activity and excrete large amounts of glutaric acid. Importantly, both subtypes are at high risk for severe neurological damage if untreated, as the level of residual enzyme activity does not reliably predict a milder clinical course without appropriate management.
Metabolic Disturbances and Brain Impact in GA1
The deficiency of the glutaryl-CoA dehydrogenase (GCDH) enzyme triggers a cascade of metabolic disturbances. Instead of being properly processed, specific amino acids and their byproducts accumulate, creating a toxic internal environment that is especially harmful to the developing brain.
These metabolic imbalances affect the brain in several critical ways:
- Neurotoxic Accumulation : The primary toxic agents are glutaric acid (GA), 3-hydroxyglutaric acid (3-OH-GA), and glutaryl-CoA, which are intermediate products of lysine, hydroxylysine, and tryptophan metabolism. Normally transient, these substances build up to damaging concentrations. They are directly neurotoxic, meaning they can injure or kill nerve cells. The brain has limited capacity to clear these acids, leading to their prolonged damaging effects, contributing to issues like oxidative stress (a type of cellular damage) and neuronal cell death in vulnerable brain regions.
- Basal Ganglia Vulnerability : The basal ganglia, a group of structures deep within the brain essential for controlling voluntary movement (including the caudate nucleus and putamen, together known as the striatum), are exceptionally susceptible to these toxic metabolites. Damage to this area, often manifesting as bilateral striatal necrosis (tissue death on both sides of the striatum), is a hallmark of GA1. This damage directly causes the characteristic severe movement disorders, such as dystonia (involuntary muscle contractions causing twisting movements) and choreoathetosis (involuntary writhing movements).
- Encephalopathic Crises and Other Brain Changes : During periods of bodily stress, such as infections, fever, or surgery, the body's metabolism accelerates (a catabolic state). This increases the breakdown of proteins and, consequently, the production of toxic intermediates. This surge can overwhelm the brain's compromised ability to cope, precipitating an acute encephalopathic crisis—a period of rapid neurological deterioration that can cause irreversible brain damage. Beyond the basal ganglia, GA1 can also lead to other brain abnormalities, including underdevelopment of the frontal and temporal lobes (frontotemporal hypoplasia) and various white matter changes, contributing to the condition's complex neurological profile.
- Secondary Carnitine Deficiency : The body attempts to detoxify and excrete excess glutaric acid by binding it to carnitine, forming glutarylcarnitine. While this is a protective mechanism, the persistent high levels of glutaric acid can deplete the body's stores of free carnitine. This results in a secondary carnitine deficiency. Carnitine is vital for energy metabolism, particularly for transporting fatty acids into mitochondria for energy production. Its deficiency can further impair energy production, potentially exacerbating muscle weakness and overall metabolic instability in individuals with GA1.
Clinical Manifestations and Symptoms of GA1
The clinical presentation of Glutaric Acidemia Type 1 can vary significantly, making it challenging to diagnose. Some infants may appear healthy at birth, while others might display subtle early signs. For many, more distinct symptoms emerge during infancy or early childhood, often triggered by common childhood illnesses.
The clinical picture of GA1 can include:
- Early Physical Signs : An unusually large head circumference (macrocephaly) is a common early indicator, observed in approximately 75% of infants with GA1, who might otherwise seem healthy. Other subtle early symptoms can include muscular hypotonia (floppy muscles), unusual irritability, or jitteriness. These initial signs can be mild and easily overlooked or misattributed if GA1 is not specifically considered or screened for.
- Acute Encephalopathic Crises : A significant challenge in GA1 is the risk of acute encephalopathic crises. These episodes of sudden neurological decline most commonly occur between 3 months and 3 years of age but have been reported up to age six. Triggers often include metabolic stress from infections (especially with fever), vaccinations, or surgery. During a crisis, a child may rapidly develop irritability, vomiting, diarrhea, loss of appetite, lethargy, and significantly reduced muscle tone. Without prompt and effective management, this can progress to severe neurological outcomes like dystonia, choreoathetosis, and coma, reflecting acute damage to the basal ganglia.
- Insidious Onset and Other Complications : Not all individuals with GA1 experience a dramatic crisis. Some may have a more gradual onset of neurological problems. Developmental regression or delays, particularly in motor skills, might be the primary concern, often without an obvious triggering illness. These individuals may slowly develop movement difficulties. Additionally, some individuals with GA1 have developed subdural or retinal hemorrhages (bleeding in the brain or eyes), which can, in tragic cases, be mistaken for non-accidental injury. This highlights the importance of considering metabolic disorders in such presentations. While new damage to the striatum is rare after age six, ongoing neurological challenges can persist.
Diagnosis, Prevalence, and Subtypes of GA1
Diagnosing Glutaric Acidemia Type 1 involves specific tests, with early detection through newborn screening being crucial for improving outcomes. While GA1 is rare globally, its frequency is notably higher in certain populations.
Understanding GA1 also involves its diagnosis, how common it is, and its biochemical variations:
- Diagnostic Methods : Newborn screening programs are vital for early GA1 detection. These programs typically use tandem mass spectrometry to identify elevated levels of glutarylcarnitine (C5DC) in a dried blood spot. A positive screening result necessitates confirmatory testing, which includes urine analysis for glutaric acid and 3-hydroxyglutaric acid, direct measurement of GCDH enzyme activity in cells (like fibroblasts or white blood cells), and molecular genetic testing of the GCDH gene to identify mutations. It's important to note that some individuals, particularly "low excretors" with less pronounced biochemical markers, might occasionally be missed by initial screening, requiring clinical vigilance if symptoms suggest GA1.
- Prevalence and Affected Populations : GA1 affects approximately 1 in 100,000 newborns worldwide, though this incidence varies. The disorder affects males and females equally. However, in specific genetic isolates (relatively closed communities often with shared ancestry), the incidence can be dramatically higher due to founder effects (reduced genetic variation stemming from a small group of ancestors). For example, in communities such as the Old Order Amish, certain First Nations groups in Canada, Irish Travellers, and specific populations in South Africa, the incidence can be as high as 1 in 250 newborns.
- Biochemical Subtypes (High and Low Excretors) : As previously mentioned, individuals with GA1 are biochemically categorized as high excretors (HE) or low excretors (LE). This classification is based on residual GCDH enzyme activity and the amount of glutaric acid excreted in urine. While both HE and LE subtypes face a similar high risk of severe neurological damage if untreated, some research suggests potential differences. HE patients might more frequently exhibit brain abnormalities beyond the striatum, have a larger head size, experience more subdural hemorrhages, and possibly face greater cognitive challenges than LE patients, even when treatment is initiated early.
