

Understanding Amish Lethal Microcephaly
Amish lethal microcephaly (MCPHA) is a rare and severe genetic disorder found almost exclusively within Old Order Amish communities. It is characterized by an extremely small head circumference at birth, a direct reflection of abnormal brain development during pregnancy. Due to the profound neurological damage, the disorder is unfortunately fatal, typically within the first year of life.
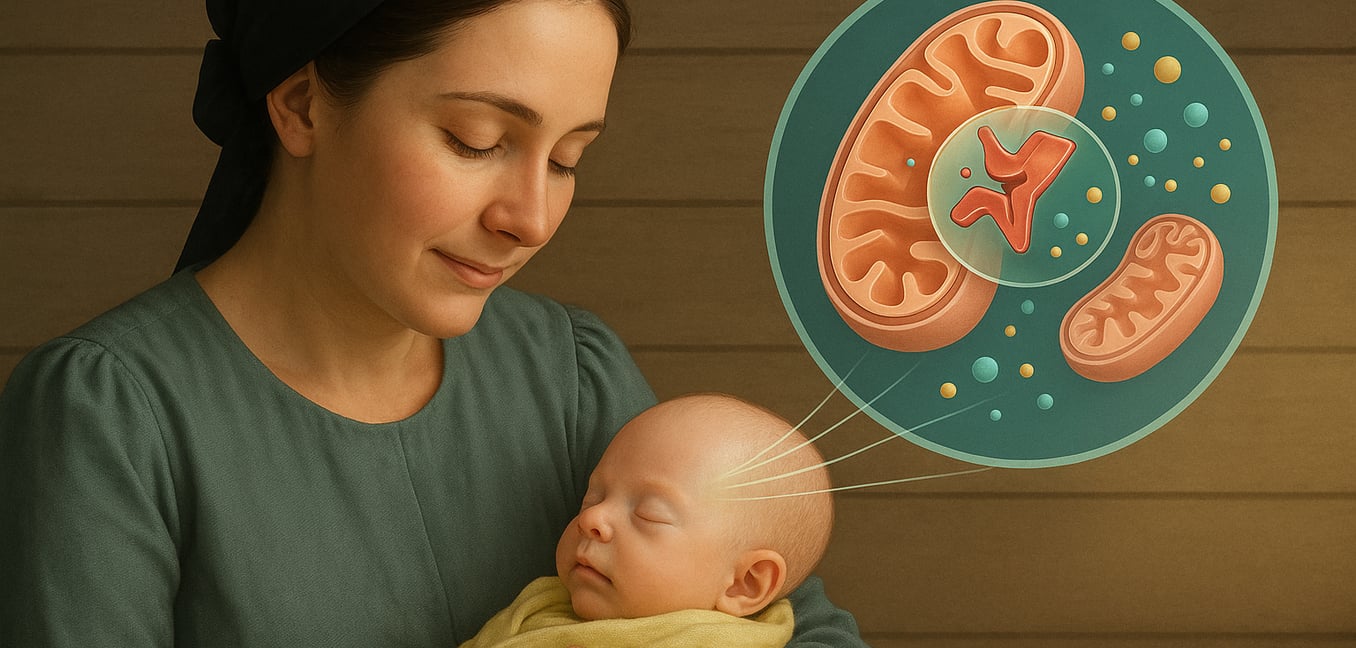
The root cause is a specific autosomal recessive mutation in the SLC25A19 gene. This means an infant must inherit a faulty copy from both parents to be affected. This gene provides the instructions for building a vital protein that acts as a gatekeeper on the inner membrane of mitochondria, our cells' energy factories. Its job is to transport thiamine pyrophosphate (TPP), the active form of vitamin B1, into the mitochondria.
In MCPHA, this transporter protein is broken. Think of it as a locked gate or a broken fuel pump for the cell’s engine. Even if the body has plenty of thiamine, it cannot reach the mitochondrial interior where it is desperately needed. This starves the mitochondria of TPP, crippling their ability to generate energy and leading to a catastrophic cellular energy crisis. This failure is particularly devastating for the developing brain, which has immense energy demands, ultimately causing the impaired growth that defines the condition.
Infants born with the disorder show profound developmental delays, seizures, and unusual muscle tone, with a weak trunk and stiff limbs.
The Search for Influential Lifestyle Factors
When facing a genetic disorder, families often look to lifestyle changes for hope. However, for MCPHA, the nature of the genetic defect severely limits the impact of such interventions. The core problem lies in a fundamental breakdown of cellular machinery that cannot be corrected by external factors.
Dietary Thiamine (Vitamin B1) Intake
A logical first thought is to wonder if high-dose thiamine supplements could overcome the metabolic blockade. After all, the issue stems from a lack of TPP, thiamine's active form. While this strategy can be effective in other, milder thiamine-related disorders, it is completely ineffective for Amish lethal microcephaly.
The fundamental problem is not a shortage of thiamine in the body, but the non-functional transporter protein. The specific mutation in MCPHA cripples this protein so severely that it cannot perform its job. Flooding the system with thiamine is futile; the essential molecule has no way to cross the mitochondrial membrane to get to where it is needed.
Specialized Metabolic Diets
For certain metabolic disorders, a high-fat, low-carbohydrate ketogenic diet can provide an alternative fuel source for the body, bypassing defective energy pathways. This approach can be used as a supportive measure in Amish lethal microcephaly to help manage a secondary symptom: the buildup of lactic acid. By providing ketones for energy, the diet reduces the body’s reliance on the blocked pathway that produces this acid.
However, this dietary change cannot resolve the underlying energy crisis, especially within the developing brain. It is a partial workaround for one symptom, not a treatment that can correct the accumulation of other toxic compounds or alter the disease's devastating progression. It remains a palliative tool, not a solution.
Symptomatic Management and Therapeutic Interventions
Given that the course of Amish lethal microcephaly cannot be altered, medical care shifts entirely away from curative attempts. The focus becomes palliative care, a comprehensive approach dedicated to providing comfort, managing symptoms, and ensuring the highest possible quality of life for the infant. The goal is not to prolong life, but to make the time the infant has as peaceful and dignified as possible.
Feeding and nutritional support are primary concerns, as severe neurological impairment makes sucking and swallowing difficult. To prevent distress from hunger and dehydration, caregivers may use specialized feeding techniques or a nasogastric tube to provide nutrition directly. This ensures the infant’s basic needs are met without the struggle of oral feeding.
Managing distressing neurological symptoms, such as sudden muscle jerks (myoclonus) and limb spasticity, is another key aspect of care. Physicians may prescribe anti-seizure medications or muscle relaxants to reduce the frequency and intensity of these movements. The objective is to minimize discomfort and allow the infant to be more settled and at peace.
The disorder also causes generalized weakness that can affect the muscles used for breathing. Supportive care focuses on non-invasive measures to make breathing easier, such as careful positioning to keep the airway clear, gentle suctioning of secretions, and sometimes providing a small amount of supplemental oxygen to reduce respiratory effort.
A critical component of care is providing robust emotional and psychosocial support for the family. A terminal diagnosis is devastating, and care teams, including social workers and counselors, work closely with parents to help them navigate their grief and the practicalities of care, fostering a loving and supportive environment.
The Complex Nature of Treating Genetic Disorders
Treating genetic disorders presents a vast spectrum of challenges, where the specific details of a mutation dictate what is medically possible. While some conditions can be managed, Amish lethal microcephaly remains beyond the reach of current interventions because its core defect creates an irreversible breakdown in a critical cellular process.
Supplementation with a missing vitamin is often a first-line strategy, but it only works if the body’s machinery can use it. In MCPHA, this approach fails. The problem is not a lack of thiamine but the non-functional transporter that acts as the sole gateway for its active form into the mitochondria. The key exists, but the keyhole is sealed.
Similarly, redirecting metabolic traffic around a genetic roadblock using specialized diets is sometimes possible. While a ketogenic diet can slightly ease one secondary symptom of MCPHA, it cannot fix the core energy deficit. The metabolic block is so central to energy production that there are no effective side roads to take; the main highway to the cell’s powerhouse is closed.
The ultimate goal for many genetic diseases is to replace the faulty protein or correct the gene itself, but this faces immense hurdles. Protein replacement therapy struggles to deliver molecules across the protective blood-brain barrier and into the correct mitochondrial compartment. More importantly, the most significant barrier is timing. The catastrophic brain damage in MCPHA occurs during fetal development, meaning any potential treatment would need to be administered in utero—a frontier of medicine still in its earliest and most complex stages.
